

The public health emergency caused by the COVID pandemic has brought the whole world to a standstill. In Kashmir, over 28,000 cases of the disease have been registered, the number is increasing by the day. The everyday increase in the number of affected people has stretched the healthcare system to its limits.
However, the current state of the healthcare system in Kashmir cannot be seen in isolation from the region’s militarised history.
The ongoing healthcare deprivation faced by the community is exacerbated by the decades of military presence in the region, the denial of justice and the obstruction to rights.
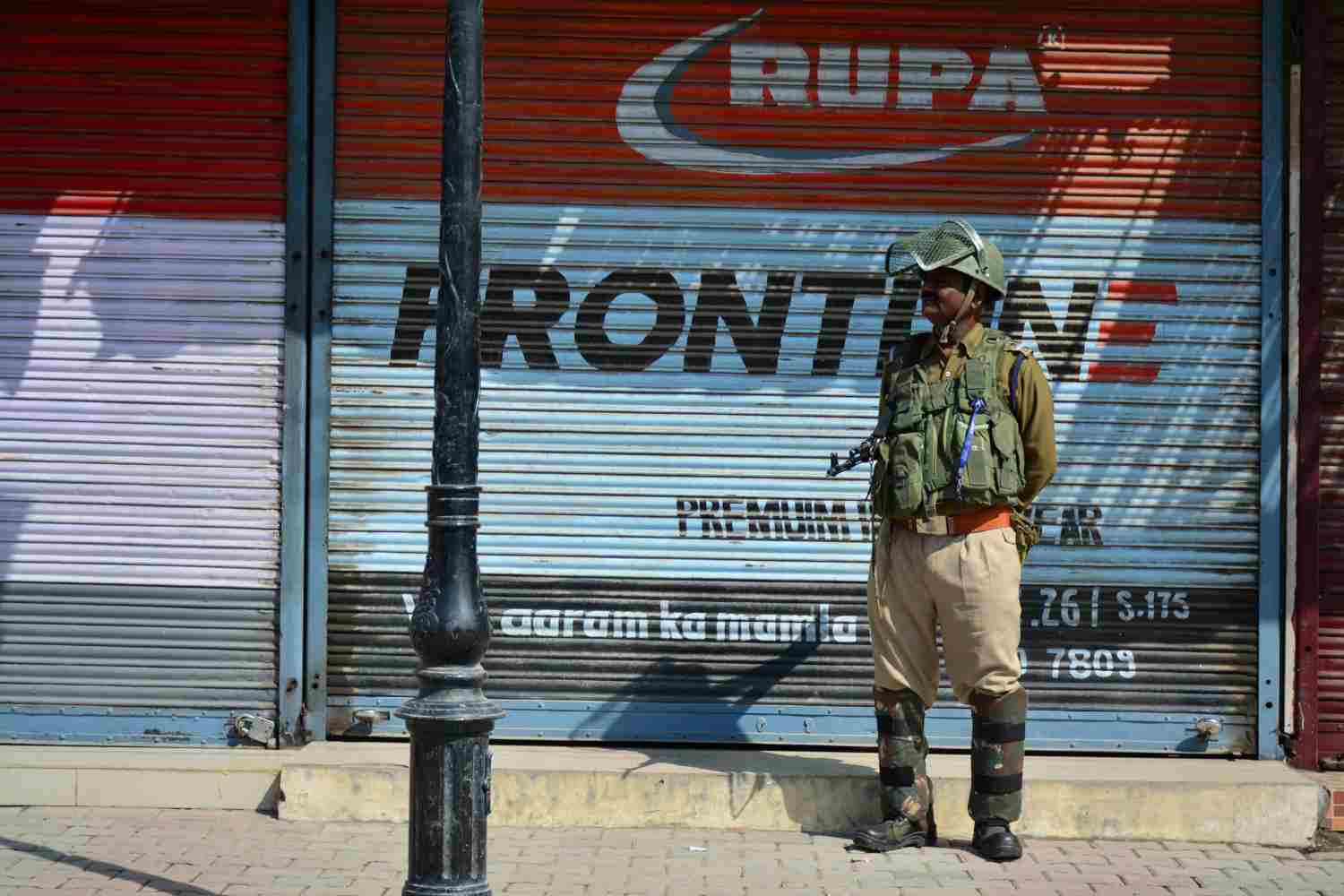
When the COVID lockdown was imposed, Kashmir was already under a military siege for 8 months.
On August 4, 2019, Kashmir and Chenab Valley were put under a complete communication clampdown, while Jammu was put under a partial blockade by the Government of India before it abrogated article 370.
The angst caused by the communication gag was compounded by the militarily enforced restriction on the movement of people. Not only did the communication gag snatch the basic right to information, but, in its form, it also manifested as a breach of other rights, like the right to healthcare.
During this lockdown, access to medical care became a strenuous task. In the absence of telephone and internet networks, people could not call ambulances or even consult doctors online.
The restrictions on movement also made it difficult for the medical staff to reach the hospitals.
Due to the restrictions on movement, several patients who required life-saving treatments like dialysis and chemotherapy found it hard to reach hospitals, and this was coupled up with a shortage of life-saving drugs during the clampdown.
The ones who had personal vehicles had to take longer and rather inconvenient routes, due to army barricades to reach the hospitals.
Many Pregnant women faced complications due to a lack of communication with doctors and hospitals.
The situation in the rural areas was even grimmer due to the already limited medical facilities. With a lack of gynaecologists, women with pregnancy-related or other emergencies, required to travel to the main city. The loss of the communication coupled with physical restrictions on the movement made it difficult for such patients to receive the immediately required medical assistance.
The delay in reaching the hospital is a loss of critical time that can sometimes be a deciding factor between life and death.
The concerns over the ramifications of the lockdown on the healthcare system were raised in medical journals like the Lancet. The restrictions in the region were called “blatant denial of the right to health care and the right to life” because they made it difficult for both the patients and the staff to reach hospitals.
However, such attention to the situation has not materialised into concrete policies to ensure smooth functioning of the healthcare system.
Instead, the Indian Medical Association condemned Lancet’s editorial.
The nature of the conflict in the region of Kashmir, where there are confrontations between armed forces and civilians, integrates the hospitals into the conflict. It is common for armed forces to arrest injured protestors at hospitals.
ALSO READ: An overworked war hospital: The blood and anger at SMHS
This not only deprives the patients of treatment but also puts the doctors and the medical staff at risk, which in turn poses long term threats to the functioning of the healthcare system in the region.
Post-August 5, 2019, Kashmir witnessed close to 500 incidents of protests. In these incidents, brute force is used by the Indian armed forces against the unarmed protestors. These include bullets, pellets, tear gas and pepper gas. Such disproportionate use of force has resulted in multiple injuries to the protesting youth.
In many instances, injured protestors have been forced to resolve to “self-treatment”, for the fear of profiling and detention at the hospitals by the armed forces. Such “treatments” in a non-sterile environment by untrained civilians can be very harmful causing skin infections or even damage to vital organs.
Such deprivation can be seen as a breach of Article 12 of the 1949 Geneva Conventions, according to which the wounded and the sick are entitled to be treated humanely without any discrimination.
The conventions clearly mention that the wounded “shall not wilfully be left without medical assistance and care, nor shall conditions exposing them to contagion or infection be created”.
The coronavirus has for sure churned the public health system, but it has also unveiled the shortcomings in the same.
India is among the top three spenders on defence. This also includes the expenses on over 7,00,000 armed men in Kashmir.
However, despite its claims of “development” in the region, India seems to have failed in equipping the healthcare system in Kashmir to deal with the public health crisis.
The doctor to patient ratio in Kashmir is 1:3,866, while the norm set by WHO is 1:1000.
There is also a limited number of ventilators available to support critically ill COVID patients.
On top of that, India continues to carry out military operations in the valley despite the UN’s call for a global ceasefire in wake of the pandemic.
The Indian army also carried out multiple gunfights in Kashmir during the lockdown.
In these operations, many houses have been burnt and people have been made homeless. This leaves the people more vulnerable to contracting the virus who are forced to take shelter in community houses or at relatives’ places.
Coronavirus has almost crunched the global health system in the past 7 months. This public health crisis has undoubtedly forced us to rethink the interconnections of the healthcare system and the socio-political conditions surrounding health.
There is an immediate need to address the COVID crisis in Kashmir, but a long term solution to the shattered public health system cannot be imagined without taking into consideration the militarisation in the region.
Misbah Haqani is an independent researcher interested in understanding the social determinants of health and the socio-political aspects surrounding healthcare in Kashmir.
Views and opinions expressed in this article are those of the author’s and do not necessarily reflect the editorial position and policy of Free Press Kashmir. Feedback and counter-views are welcome at [email protected].
Free Press Kashmir is now on Telegram. Click here to Join.












